Avicenna J Environ Health Eng. 11(2):104-114.
doi: 10.34172/ajehe.5434
Systematic Review
Air Pollution Exposure and COVID-19 Outcomes: A Systematic Review and Meta-analysis of Short- and Long-term Effects
Marzieh Fattahi-Darghlou 1, 2  , Hoda Arabzadeh 1, Younes Mohammadi 2, 3, *
, Hoda Arabzadeh 1, Younes Mohammadi 2, 3, *
Author information:
1Student Research Committee, Hamadan University of Medical Sciences, Hamadan, Iran
2Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
3Modeling of Noncommunicable Diseases Research Center, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Our objective was to determine the relationship between short-term and long-term exposure to air pollution and COVID-19 mortality and morbidity through a systematic review and meta-analysis. To do so, Scopus, PubMed, and Web of Science databases were searched for original studies up to February 1, 2023. Observational studies reporting risk estimates for the association between air pollution exposure and COVID-19 outcomes were included. The methodological quality of the selected articles was assessed using the Newcastle-Ottawa scale (NOS). Pooled estimates were calculated using a random effects model. We employed the I2 statistic and chi-square test to assess heterogeneity among studies. Egger’s and Begg’s tests were used to evaluate potential publication bias. A total of 2823 articles were identified in the initial database search. After screening, 12 studies met the inclusion criteria and were included in the meta-analysis. The results indicated a significant association between PM10 and O3 exposure and COVID-19 mortality, with relative risks of 1.02 (95% confidence interval: 1.01 to 1.04) and 1.09 (95% confidence interval: 1.04 to 1.14), respectively. Our meta-analysis suggests that exposure to O3 and PM10 is associated with an increased risk of COVID-19 mortality. Additionally, the study found a significant link between exposure to NO2, PM2.5, and PM10 and increased COVID-19 mortality, with PM2.5 showing the strongest association. These findings underscore the need for effective policies to mitigate the health impacts of air pollution and highlight the importance of integrated strategies to address the broader effects of climate change.
Keywords: Air pollution, COVID-19, Nitrogen dioxide, Mortality, Morbidity, Systematic reviews,
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Fattahi Darghlou M, Arabzadeh H, Mohammadi Y. Air pollution exposure and COVID-19 outcomes: a systematic review and meta-analysis of short- and long-term effects. Avicenna J Environ Health Eng. 2024;11(2):104-114. doi:10.34172/ajehe.5434
1. Introduction
The coronavirus disease 2019 (COVID-19) first emerged in Wuhan, China, in December 2019 (1). As of August 5, 2022, there have been millions of confirmed cases of COVID-19 and over 6 million related deaths worldwide (2). Patients with COVID-19 often experience acute respiratory distress syndrome (ADRS) or other serious conditions (3). It is important to identify factors that may increase the risk of mortality from COVID-19, including medical history, lifestyle factors, and environmental risk factors such as weather indicators and air pollutants (4-6). It has been hypothesized that short- and long-term exposure to air pollution may increase COVID-19 mortality and morbidity rates (5,7,8). Although the epidemiology of COVID-19 is evolving, there is considerable overlap between the causes of death in COVID-19 patients and conditions caused by and/or exacerbated by long-term exposure to fine particulate matter (PM2.5). PM2.5 contains microscopic solids or liquid droplets small enough to be inhaled and cause serious health problems. The Global Burden of Disease Study has identified air pollution as a risk factor for overall mortality and cardiovascular disease, and it is believed to have contributed to an estimated 5 million premature deaths worldwide in 2017 alone (9). According to the World Health Organization (WHO), air pollution is responsible for 7 million deaths annually worldwide. Almost half of them will die from ischemic heart disease or stroke caused by exposure to air pollution, making air pollution more important than other modifiable cardiovascular risk factors such as smoking, blood pressure, blood lipids, and diabetes. For these reasons, we hypothesize that air pollution may worsen the prognosis of COVID-19 patients by exacerbating underlying cardiovascular or respiratory diseases and suppressing immune responses (10). The main air pollutants include particulate matter (PM2.5 and PM10), carbon monoxide (CO), carbon dioxide (CO2), and nitrogen-based substances (NOx) (11). Recent studies have shown a link between exposure to air pollution and mortality from COVID-19 (12). Some studies have also investigated the relationship between COVID-19 mortality and long-term exposure to fine particles such as PM2.5, PM10, O3, NO2, and CO, reporting a direct relationship between them (13-15). In some studies, the effects of several unspecified pollutants have been reported (12); however, a non-significant relationship has been reported for pollutants in others (1,11,16). The aim of this meta-analysis is to investigate possible associations between short- and long-term exposure to air pollution and COVID-19 mortality and morbidity. This association has been previously investigated in epidemiological studies; however, to the best of our knowledge, this is the first systematic review and meta-analysis to date.
2. Materials and Methods
2.1. Eligibility Criteria (PICOS)
The eligibility criteria are as follows:
-
Population: The general population of society regardless of race, age, and gender.
-
Exposure: Short-term and long-term exposure to air pollutants.
-
Control: The control group consisted of people who were not exposed to air pollutants.
-
Outcome: The outcome of the study is mortality and morbidity from COVID-19.
-
Studies: Observational studies (retrospective or prospective cohort) and ecological studies were included in the analysis regardless of their publication time, publication status, and language.
2.2. Exclusion Criteria
The exclusion criteria were as follows:
-
Clinical studies, in vitro studies, and animal studies were excluded.
-
Studies not fully available in the database were excluded.
-
Article reporting only abstracts were also excluded.
-
Studies not reporting RR, OR, and HR with 95% CI were also excluded.
2.3. Information Sources and Search
The present meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (17). A comprehensive literature search was conducted in PubMed, Scopus, and Web of Science databases up to February 1, 2023, utilizing a systematic combination of keywords related to exposure type, health outcomes, and population characteristics. The search strategy employed a combination of Medical Subject Headings (MeSH) terms, as follows: ((PM2.5 OR PM10 OR SO2 OR NO2 OR O3 OR CO) AND (air pollution)) AND ((morbidity OR mortality OR death OR incidence OR risk)) AND (COVID-19). Furthermore, a thorough review of the reference lists of included studies was performed to identify any additional studies that met the predetermined inclusion criteria.
2.4. Study Selection
The studies were imported into document management software (Endnote, version X8, Thomson Scientific, Stamford, Connecticut, USA), and duplicates were removed. Two investigators (MFD and HA) independently screened the titles and abstracts of all the remaining articles that met the eligibility criteria and excluded those that were not eligible. Any disagreements between the researchers were resolved by a third reviewer (YM). Then, the full text of the studies was examined to determine their eligibility for inclusion in the meta-analysis.
2.5. Data Extraction
Data extraction was independently conducted by both researchers. The extracted information for eligible studies was collected using Stata software. The extracted data included the first author’s name, publication year, country, type of study, type of pollutant (PM2.5, MP10, SO2, NOX, NO2, O3, CO), type of outcome (morbidity and mortality), result (increase and decrease), duration of exposure (short-term and long-term), effect size (RR, HR, and OR) with 95% confidence interval, and quality of studies.
2.6. Methodological Quality
The quality of the studies was evaluated using the NOS to reduce bias (18). The NOS provides a checklist of important items for judging bias in studies. In the NOS, a set of items about the selection of study participants, comparability of groups, and evaluation of exposure/outcome were assessed.
2.7. Assessment of Heterogeneity and Publication Bias
We used the I2 statistic (19) and chi-square test (20) to assess heterogeneity between studies. The degree of heterogeneity was assessed based on the I2 value, with values of < 50%, 50%-74%, and ≥ 75% indicating low, moderate, and high heterogeneity (20). To evaluate the publication bias, Egger’s test (21) and Begg’s test (22) were used, along with the trim-and-fill analysis (23).
2.8. Statistical Analysis
The study examined the morbidity and mortality associated with COVID-19 and their relationship with various risk factors, including PM2.5, PM10, SO2, NOX, NO2, O3, and CO. The risk ratio (RR) was utilized to quantify these relationships, with all results estimated at a 95% confidence level. To calculate the RRs from the included studies, random effects models were employed to assess potential heterogeneity. Data analysis was performed using Stata software version 14 (StataCorp, College Station, TX, USA).
3. Results and Discussion
3.1. Study Selection and Characteristics
Fig. 1 depicts the PRISMA flowchart for the literature search and selection process. Initially, 2823 articles were identified from database searches conducted up to May 21, 2022, with 733 articles from PubMed, 279 from Web of Science, and 1811 from Scopus. After removing duplicates, 2202 articles were screened, and 12 articles met the inclusion criteria. No additional relevant studies were identified through the reference lists of the eligible articles (14,16,24-33).
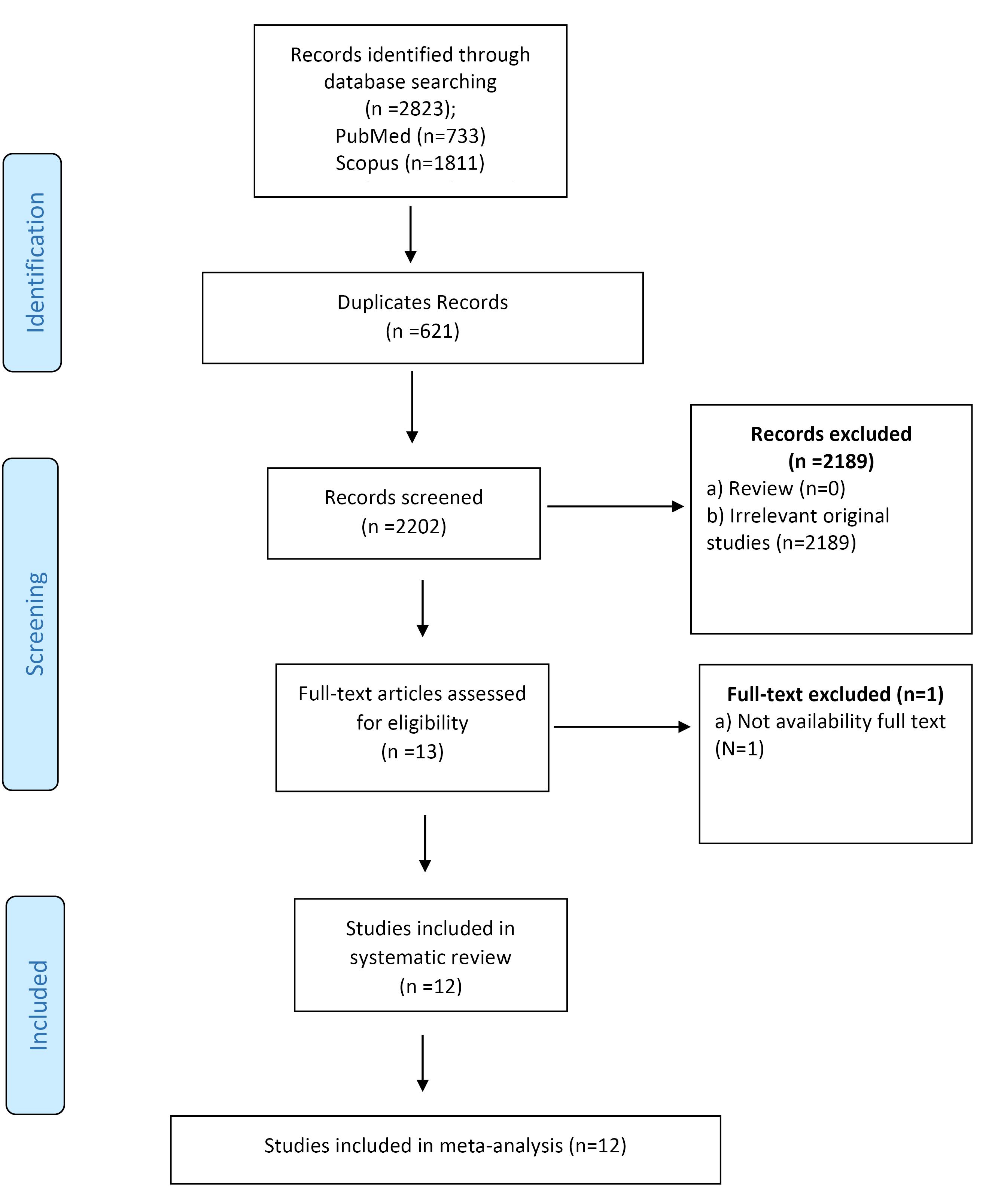
Fig. 1.
The Flowchart of the Study Selection Process
.
The Flowchart of the Study Selection Process
3.2. Study Characteristics
Table 1 summarizes the characteristics of the studies included in the systematic review. The majority of the included articles were conducted in the Americas, with a focus on countries in North and South America. The publication dates of the included articles ranged from 2020 to 2022, reflecting the rapid pace of research on COVID-19 during this period. The study designs were predominantly observational, with a preponderance of ecological studies that examined the associations between air pollutant exposure and COVID-19 mortality. Notably, the vast majority of studies investigated the relationship between air pollution exposure and COVID-19 mortality and morbidity, with a focus on both male and female populations. All included studies were published in English, facilitating a comprehensive synthesis of the existing literature.
Table 1.
Characteristics of Studies Included in the Systematic Review
|
ID
|
1st Author
|
Country
|
Study
|
Outcome
|
Pollutant
|
Effect size
|
Result
|
Point Estimate
|
Lower Limit
|
Upper Limit
|
Exposure
|
Quality Score
|
| 1 |
Coker ES, 2020 (14) |
Italy |
Ecological |
Mortality |
PM2.5 |
RR |
Increase |
0.09 |
0.06 |
0.12 |
Long-term exposure |
****** |
| 2 |
Valdés Salgado M, 2020 (16) |
|
|
Morbidity |
PM2.5 |
RR |
Increase |
1.004 |
0.996 |
1.011 |
Long-term exposure |
******* |
| 2 |
Valdés Salgado M, 2020 (16) |
Chile |
Ecological |
Morbidity |
PM10 |
RR |
Increase |
1.003 |
0.999 |
1.008 |
Long-term exposure |
******* |
| 2 |
Valdés Salgado M, 2020 (16) |
|
|
Mortality |
PM10 |
RR |
Non-significant |
1.009 |
1.007 |
1.011 |
Long-term exposure |
******* |
| 2 |
Valdés Salgado M, 2020 (16) |
|
|
Mortality |
PM2.5 |
RR |
Non-significant |
1.012 |
1.008 |
1.017 |
Long-term exposure |
******* |
| 3 |
Aloisi V, 2021 (24) |
Italy |
Ecological |
Mortality |
PM2.5 |
RR |
Increase |
1.09 |
1.065 |
1.116 |
Long-term exposure |
****** |
| 4 |
Dales R, 2021 (25) |
USA |
Ecological |
Mortality |
PM2.5 |
RR |
Increase |
1.058 |
1.034 |
1.082 |
Short-term exposure |
******* |
| 4 |
Dales R, 2021 (25) |
|
|
Mortality |
NO2 |
RR |
Increase |
1.067 |
1.023 |
1.103 |
Short-term exposure |
******* |
| 4 |
Dales R, 2021 (25) |
|
|
Mortality |
CO |
RR |
Increase |
1.061 |
1.033 |
1.089 |
Short-term exposure |
******* |
| 5 |
De Angelis E, 2021 (26) |
Italy |
Ecological |
Mortality |
PM2.5 |
RR |
Increase |
1.58 |
1.31 |
1.9 |
Long-term exposure |
******* |
| 5 |
De Angelis E, 2021 (26) |
|
|
Morbidity |
NO2 |
RR |
Inverse |
0.95 |
0.89 |
1 |
Long-term exposure |
******* |
| 5 |
De Angelis E, 2021 (26) |
|
|
Mortality |
PM10 |
RR |
Increase |
1.34 |
1.16 |
1.55 |
Long-term exposure |
******* |
| 5 |
De Angelis E, 2021 (26) |
|
|
Mortality |
NO2 |
RR |
Inverse |
0.93 |
0.88 |
0.99 |
Long-term exposure |
******* |
| 6 |
Garcia E, 2022 (27) |
USA |
Ecological |
Mortality |
NO2 |
RR |
Increase |
1.06 |
1.02 |
1.1 |
Long-term exposure |
******* |
| 6 |
Garcia E, 2022 (27) |
|
|
Mortality |
PM2.5 |
RR |
Increase |
1.13 |
1.09 |
1.17 |
Long-term exposure |
******* |
| 6 |
Garcia E, 2022 (27) |
|
|
Mortality |
PM10 |
RR |
Increase |
1.16 |
1.11 |
1.21 |
Long-term exposure |
******* |
| 6 |
Garcia E, 2022 (27) |
|
|
Mortality |
O3 |
RR |
Increase |
1.09 |
1.04 |
1.14 |
Long-term exposure |
******* |
| 7 |
Hadei M, 2021 (28) |
Iran |
Ecological |
Mortality |
PM10 |
RR |
Increase |
1.06 |
0.93 |
1.19 |
Short-term exposure |
******** |
| 7 |
Hadei M, 2021 (28) |
|
|
Mortality |
PM2.5 |
RR |
Increase |
1.06 |
0.99 |
1.13 |
Short-term exposure |
******** |
| 7 |
Hadei M, 2021 (28) |
|
|
Mortality |
O3 |
RR |
Increase |
1.07 |
0.84 |
1.31 |
Short-term exposure |
******** |
| 7 |
Hadei M, 2021 (28) |
|
|
Mortality |
NO2 |
RR |
Increase |
1.15 |
0.93 |
1.38 |
Short-term exposure |
******** |
| 8 |
Hu H, 2021 (29) |
USA |
Ecological |
Mortality |
NO2 |
RR |
Increase |
1.19 |
1.13 |
1.26 |
Long term exposure |
******* |
| 9 |
Meo SA, 2021 (30) |
USA |
Ecological |
Mortality |
PM2.5 |
OR |
Increase |
1.068 |
1.059 |
1.077 |
Long-term exposure |
******* |
| 9 |
Meo SA, 2021 (30) |
|
|
Mortality |
CO |
OR |
Increase |
1.476 |
1.336 |
1.632 |
Long-term exposure |
******* |
| 9 |
Meo SA, 2021 (30) |
|
|
Mortality |
O3 |
OR |
Increase |
1.025 |
1.015 |
1.036 |
Long-term exposure |
******* |
| 10 |
Petroni M, 2020 (31) |
USA |
Ecological |
Mortality |
PM2.5 |
RR |
Increase |
1.09 |
1.01 |
1.18 |
Long-term exposure |
******* |
| 11 |
Sanchez-Piedra C, 2021 (32) |
Spain |
Ecological |
Mortality |
PM2.5 |
RR |
Increase |
1.016 |
1.007 |
1.026 |
Long-term exposure |
******* |
| 11 |
Sanchez-Piedra C, 2021 (32) |
|
|
Mortality |
NO2 |
RR |
Increase |
1.066 |
1.058 |
1.075 |
Long-term exposure |
******* |
| 12 |
Tian F, 2021 (33) |
China |
Retrospective cohort |
Mortality |
PM2.5 |
HR |
Increase |
1.11 |
1.09 |
1.13 |
Short-term exposure |
****** |
| 12 |
Tian F, 2021 (33) |
|
|
Mortality |
PM10 |
HR |
Increase |
1.1 |
1.08 |
1.13 |
Short-term exposure |
****** |
| 12 |
Tian F, 2021 (33) |
|
|
Mortality |
NO2 |
HR |
Increase |
1.27 |
1.19 |
1.35 |
Short-term exposure |
****** |
| 12 |
Tian F, 2021 (33) |
|
|
Mortality |
O3 |
HR |
Increase |
1.09 |
1.03 |
1.14 |
Short-term exposure |
****** |
| 12 |
Tian F, 2021 (33) |
|
|
Mortality |
SO2 |
HR |
Increase |
1.1 |
0.95 |
1.27 |
Short-term exposure |
****** |
3.3. Overall Meta-analysis Results
Fig. 2 illustrates the characteristics of the studies included in the meta-analysis, examining both long-term and short-term exposure to NO2 and its impact on COVID-19 mortality. The results indicated no significant association between NO2 exposure and COVID-19 mortality, with a relative risk of 1.05 (95% confidence interval: 1.00 to 1.10) and an I2 value of 89.00 (P < 0.001).
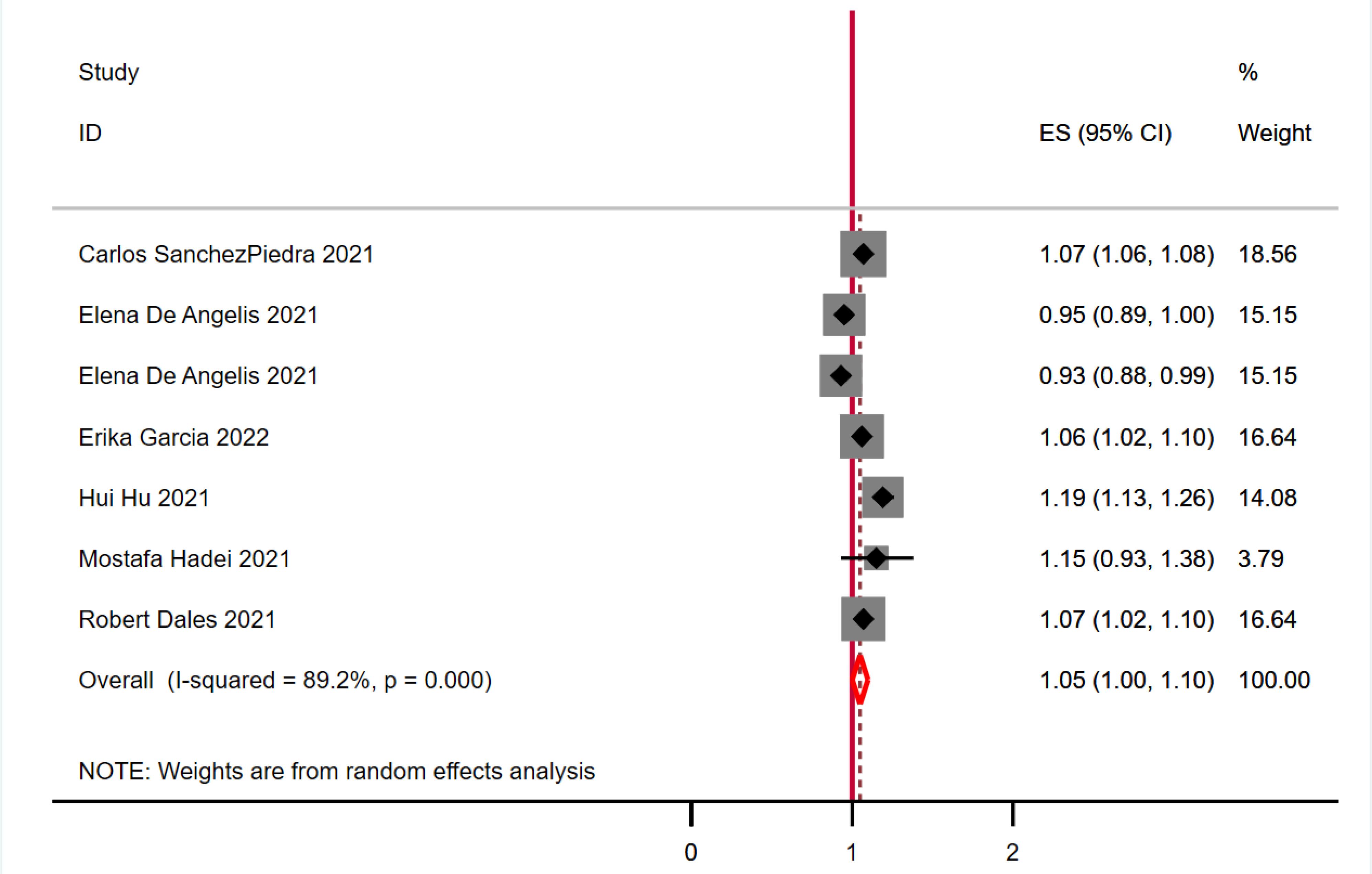
Fig. 2.
Meta-analysis of Long-term and Short-term Exposure to NO2 and Mortality of COVID-19
.
Meta-analysis of Long-term and Short-term Exposure to NO2 and Mortality of COVID-19
Fig. 3 presents the findings from the meta-analysis of 10 studies investigating the effects of both long-term and short-term exposure to PM2.5 on COVID-19 mortality. The analysis revealed no statistically significant association between PM2.5 exposure and COVID-19 mortality, with a relative risk of 0.98 (95% confidence interval: 0.89 to 1.07) and an I2 value of 99.80 (P < 0.001).
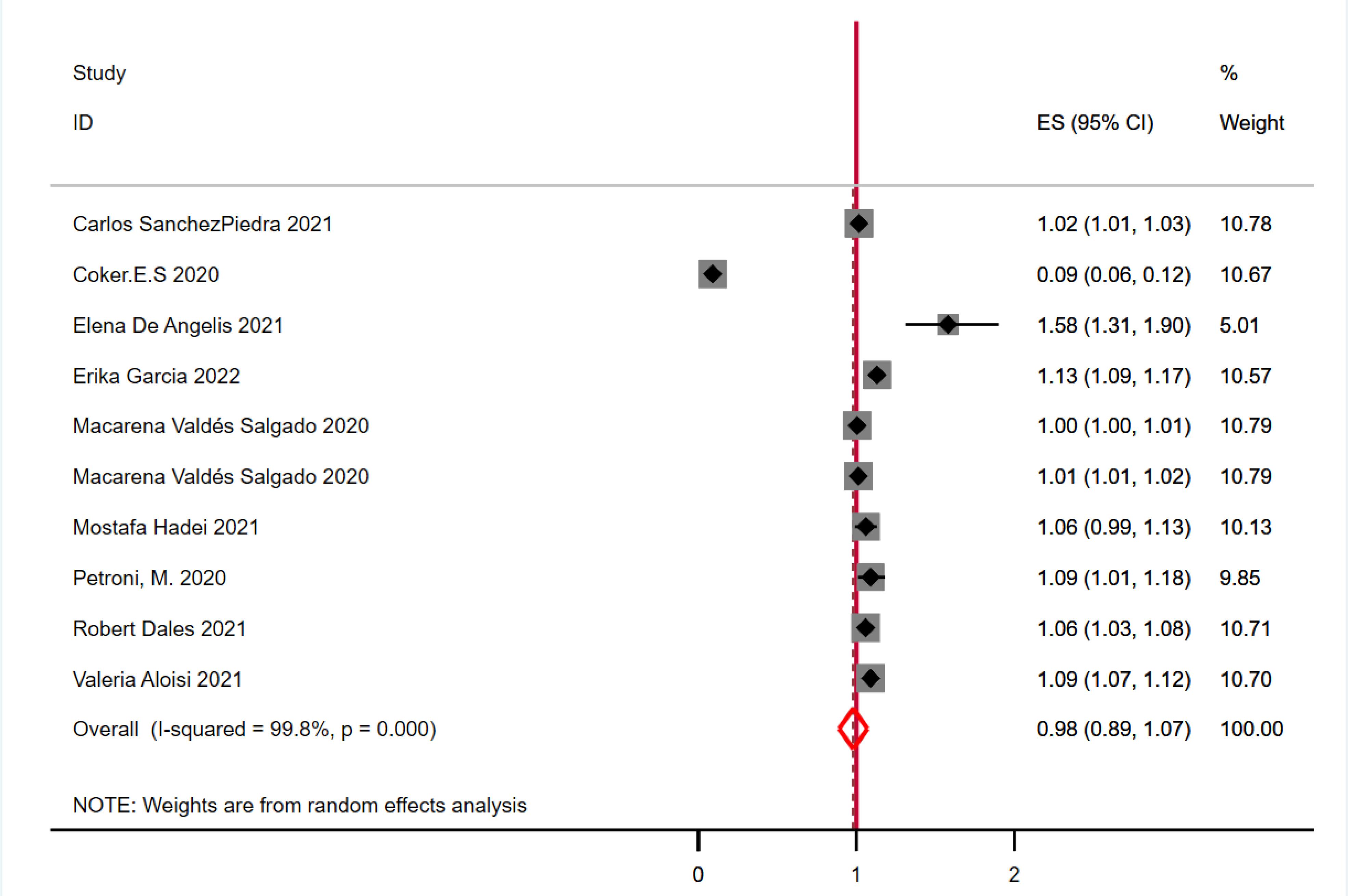
Fig. 3.
Meta-analysis of Long-term and Short-term Exposure to PM2.5 and Mortality of COVID-19
.
Meta-analysis of Long-term and Short-term Exposure to PM2.5 and Mortality of COVID-19
Fig. 4 showcases the results of a meta-analysis that investigated the relationship between both long-term and short-term exposure to particulate matter with a diameter of 10 μm or less (PM10) and COVID-19 mortality, based on data from 10 studies. The analysis identified a statistically significant link between PM10 exposure and COVID-19 mortality, with a relative risk of 1.02 (95% confidence interval: 1.01 to 1.04) and considerable heterogeneity (I2 = 92.40, P < 0.001).
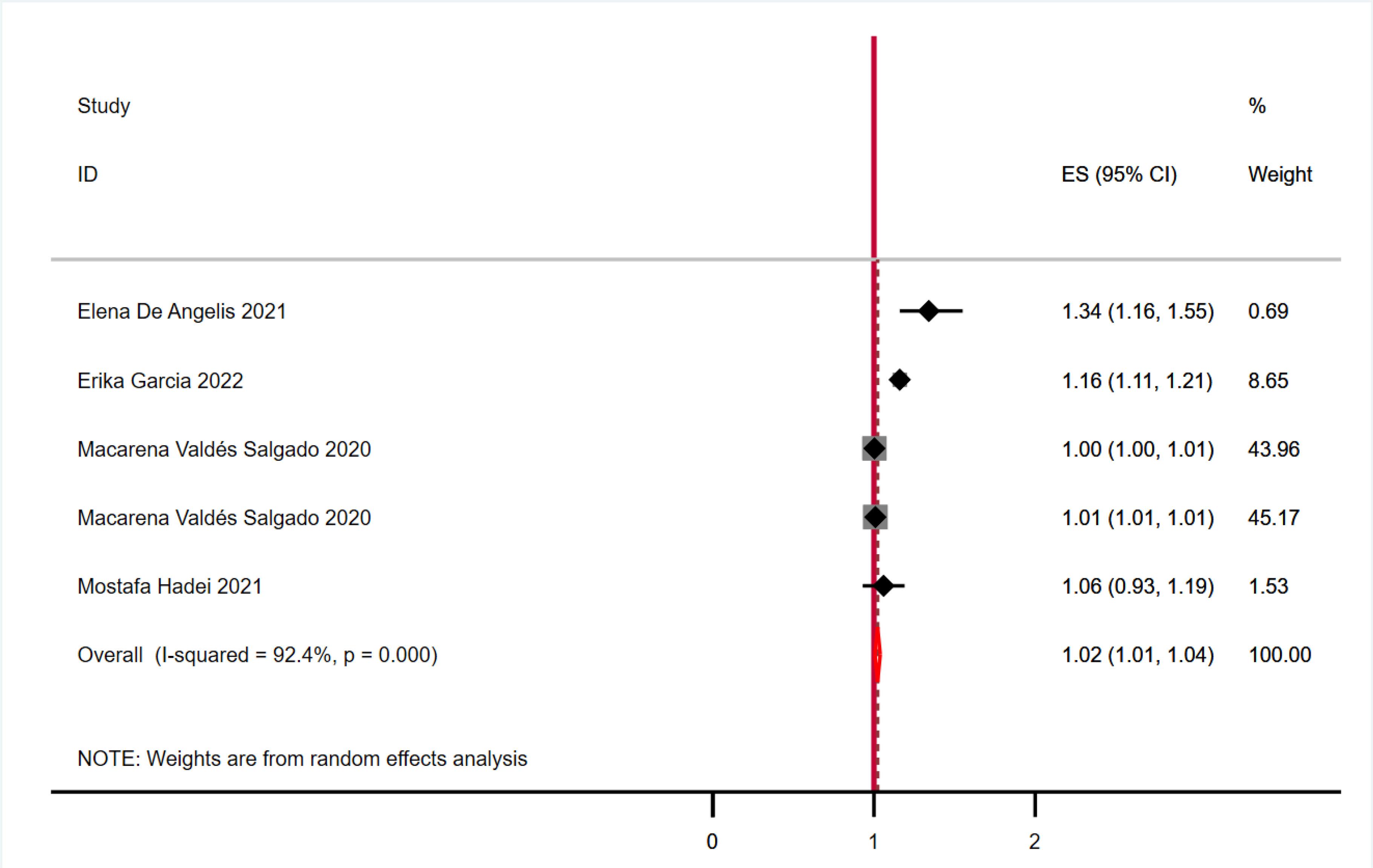
Fig. 4.
Meta-analysis of Long-term and Short-term Exposure to PM10 and Mortality of COVID-19
.
Meta-analysis of Long-term and Short-term Exposure to PM10 and Mortality of COVID-19
Fig. 5 displays the outcomes of our meta-analysis, which explored the correlation between both long-term and short-term exposure to ozone (O3) and COVID-19 mortality, based on data from 10 studies. The analysis identified a statistically significant link between PM10 exposure and COVID-19 mortality, with a relative risk of 1.09 (95% confidence interval: 1.04 to 1.14). The heterogeneity measure (I2) was 0.0, with a P value of 0.870, indicating no significant variability among the studies included.
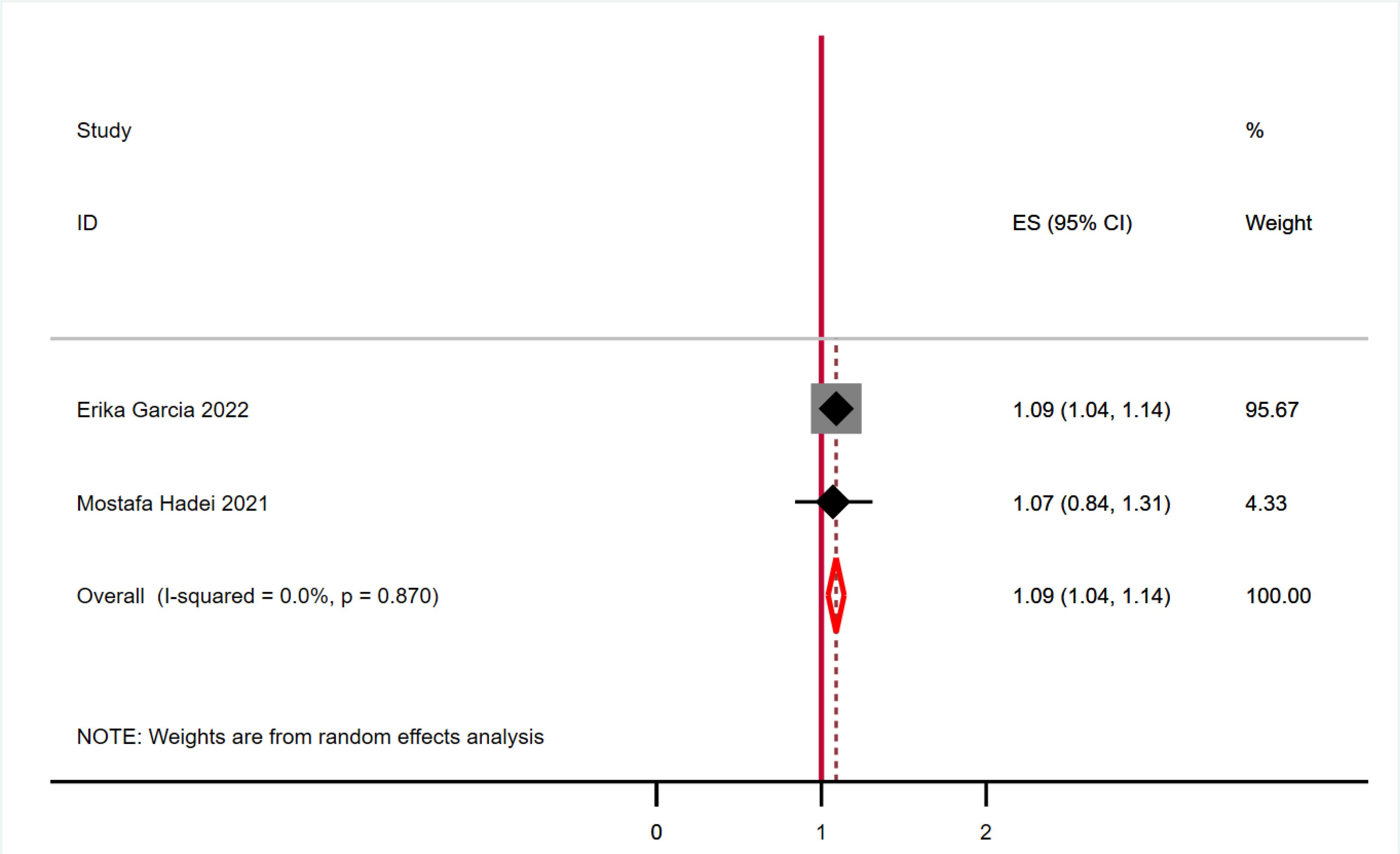
Fig. 5.
Meta-analysis of Long-term and Short-term Exposure to O3 and Mortality of COVID-19
.
Meta-analysis of Long-term and Short-term Exposure to O3 and Mortality of COVID-19
3.4. Publication Bias and Quality Assessment
The results of both Begg’s test (P = 0.53) and Egger’s test (P = 0.69) did not indicate significant publication bias for the association between long-term and short-term exposure to PM2.5 and COVID-19 mortality, as shown in Fig. 6. Similarly, Begg’s test (P = 0.62) and Egger’s test (P = 0.21) did not reveal significant publication bias for the relationship between long-term and short-term exposure to PM10 and COVID-19 mortality, as illustrated in Fig. 6. For ozone (O3) exposure, Begg’s test (P = 0.32) and Egger’s test (P = 0.15) indicated no significant publication bias in the context of long-term and short-term exposure and COVID-19 mortality, as depicted in Fig. 6. Lastly, the results of Begg’s test (P = 0.26) and Egger’s test (P = 0.65) did not show significant publication bias for the association between long-term and short-term exposure to NO2 and COVID-19 mortality, as illustrated in Fig. 6. Three of the studies had a low quality and 9 studies had high quality (Table 1).
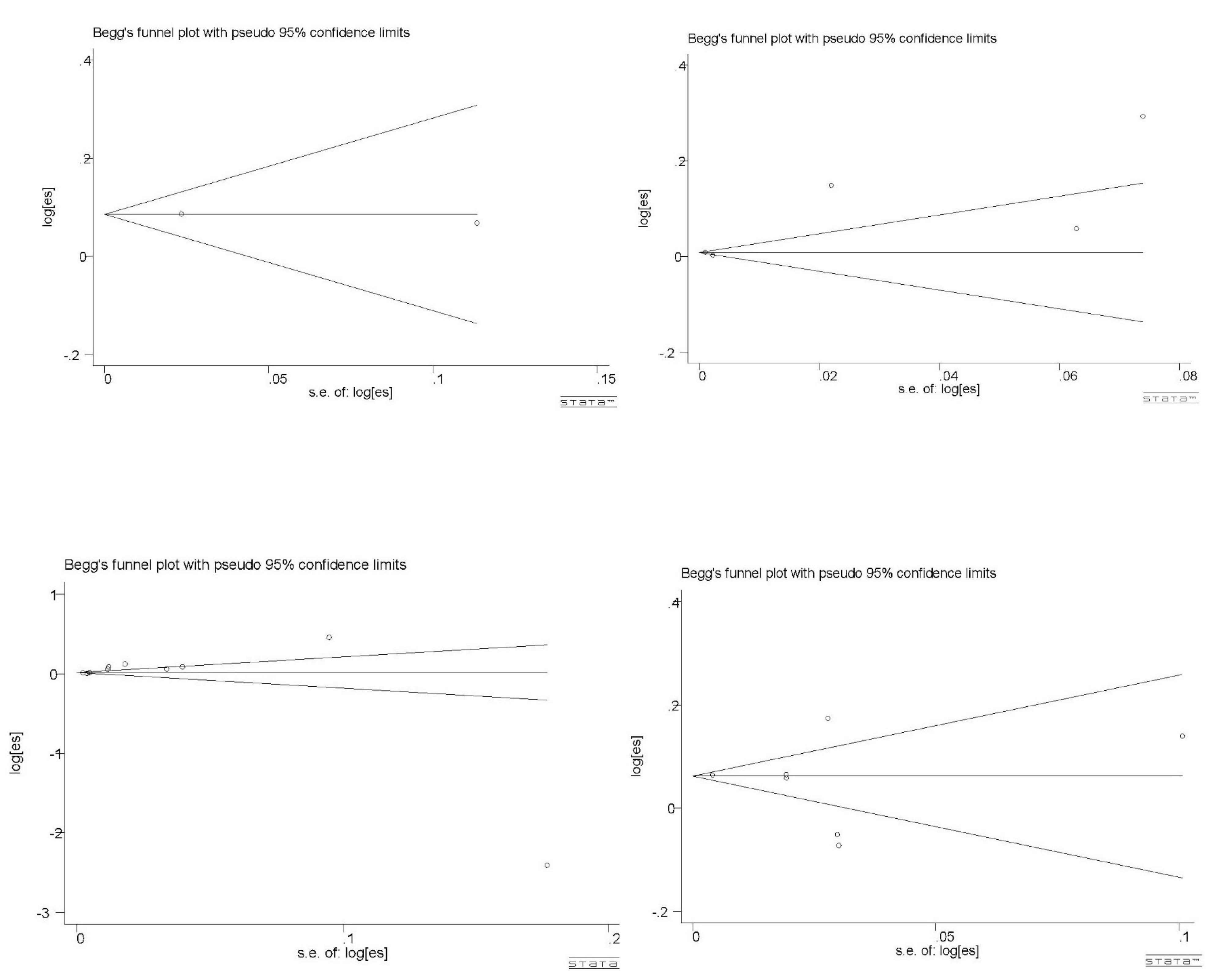
Fig. 6.
Funnel Plot of Included Studies Assessing Long-term and Short-term Exposure to Air Pollution and Mortality of COVID-19
.
Funnel Plot of Included Studies Assessing Long-term and Short-term Exposure to Air Pollution and Mortality of COVID-19
This comprehensive meta-analysis demonstrated a significant relationship between both short and long-term exposure to major air pollutants, including nitrogen dioxide (NO2), fine particulate matter (PM2.5), and coarse particulate matter (PM10), and an increased risk of mortality among COVID-19 patients. Of the pollutants examined, PM2.5 exhibited the most pronounced association with elevated relative risk of COVID-19 mortality. Specifically, the small diameter of PM2.5 enables deposition deeper into the tracheobronchial and alveolar regions of the respiratory tract, which leads to heightened oxidative stress and inflammation in the small airways and alveoli (34). Furthermore, the substantial surface area of PM2.5 relative to its mass significantly enhances its capacity to adsorb and transport toxic organic compounds, metals, nitrates, and sulfates into lung tissue (35). Meanwhile, PM10 particles predominantly deposit in the extrathoracic and upper tracheobronchial regions, with lower fractional deposition deeper in the lungs, limiting long-term impacts on pulmonary health (36). The inflammatory effects in the upper airways contribute to the observed increase in admissions for respiratory infections such as pneumonia. However, PM10 demonstrates weaker associations with mortality and chronic lower respiratory diseases relative to the pronounced impacts of PM2.5 exposures over months to years (37). The findings of the study by Sarvi et al, which was conducted to predict the number of PM2.5 exceedance days in Tehran, Iran, from October 2010 to December 2015, showed that PM2.5 as an important indicator of air pollution can lead to lung and respiratory problems in people (38). In addition to particle size, the chemical composition of particulate matter importantly determines pathophysiological responses. For instance, particulate matter rich in metals can damage proteins and lipid membranes in the lung lining through oxidative stress pathways (39). Nitrate-rich particles also heighten oxidant capacity while sulfate-laden particles promote rapid shifts in pH within lung cells. Across urban areas globally, combustion byproducts constitute a substantial fraction of fine and ultrafine particulate matter, enhancing harm (40). Meanwhile, as a strong oxidant, NO2 can directly damage lung tissue through oxidative stress mechanisms, underlying the observed mortality risks associated with short- and long-term exposure. Specifically, increased free radical generation elicited by NO2 leads to lipid peroxidation and cleavage of DNA and proteins critical for normal tissue homeostasis and cellular metabolism (41).
The mechanisms responsible for the synergistic effects of air pollutants and COVID-19 on mortality encompass both direct and indirect pathways. Irritant particles and gases cause injury and inflammation which impairs innate immune defenses in the respiratory tract (42). This allows greater viral propagation and increased risk of secondary bacterial infections, major sources of morbidity. Particulates and oxidant gases also attack and degrade surfactant lipids and proteins essential for stabilizing alveoli, which are the primary sites of severe COVID-19 infection. This surfactant dysfunction reduces lung compliance and gas exchange and heightens damage from inflammatory cell activation (43). Furthermore, pollutants upregulate ACE-2 receptors, which SARS-CoV-2 utilizes to gain entry into lung cells and vascular endothelium (44). While research elucidating the influence of specific air contaminants on ACE-2 expression is still emerging, existing evidence in both human and animal models indicates that particulate matter, its constituents, and gaseous pollutants modulate ACE-2 levels through activation of oxidative stress-responsive transcription factors (45). Hence, communities chronically exposed to appreciable air pollution likely harbor increased ACE-2 levels, thereby setting the stage for more severe COVID-19 infection (46).
At the population level, areas with high air contamination typically shoulder greater respiratory disease burdens, including higher rates of asthma, chronic obstructive pulmonary disease (COPD), pulmonary fibrosis, and lung cancer (47). By exacerbating these pre-existing conditions through repeated exposure to irritants, air pollutants render residents more susceptible to critical COVID-19 progression marked by hospitalization, ventilator support requirements, admission to intensive care units, and mortality (48). Those suffering from chronic respiratory diseases often present long-term architectural distortion or destruction of the lung coupled with impeded clearance. On this vulnerable substrate, the additive insults of SARS-CoV-2 infection frequently result in life-threatening ARDS as well as secondary lung injuries like pneumothorax (49). Indeed, extensive literature predating the COVID-19 pandemic clearly demonstrates major links between exposure to all the key air pollutants, particulate matter (PM2.5, PM10), NO2, and ozone, and increased incidence as well as exacerbation of chronic lower respiratory diseases (50). Long-term exposure to PM2.5 and NO2 strongly correlates with COPD incidence, while even short-term elevations in particulate matter pollution increase hospital admissions for diverse respiratory illnesses (51). This includes increased emergency room visits and hospitalizations for pneumonia, asthma attacks, and COPD exacerbations requiring steroids or oxygen therapy, and worsened pulmonary function among the elderly (52). The associations between particulate matter pollution and detrimental pediatric respiratory health effects have also been clearly established through natural experiments and longitudinal cohort studies. Beyond pulmonary conditions, cardiovascular endpoints like ischemic heart disease demonstrate similar associations with long-term exposure to PM2.5 in particular. The collective evidence underscores the negative impact of air pollution across populations (53).
Hence, individuals with chronic lung diseases often endure accelerated declines in pulmonary function and diminished immunity, which can increase the risk of severe COVID-19 and mortality when the air quality is poor (54). Through meta-analysis, Li et al reported that COPD patients are five times more likely to have severe COVID-19 infection relative to those without the condition. The risk is three times higher in patients with asthma (55). Even mild-to-moderate COPD, the most common form, has been linked with doubled mortality odds. Though further research is still needed, initial reports also indicate increased COVID-19 case fatality among US counties with elevated particulate matter pollution, even after adjusting for differences in socioeconomic status and access to healthcare resources between regions (56). Demographic and geographic factors may account for some of the variability in relative risk estimates across the studies analyzed in the meta-analysis. Older males with pre-existing cardiorespiratory conditions are at higher baseline risk for adverse COVID-19 outcomes independent of air pollution; hence, they may be disproportionately vulnerable to synergistic effects with pollutants (57). Regional differences in the composition and concentration of the pollutants also modulate health impacts as described earlier. However, the consistency in overall core findings from this meta-analysis emphasizes that air pollution exposure remains a significant predictor of worsened COVID-19 severity and mortality, even after adjustment for critical confounding variables like age and comorbidities across cohorts (58). The implications of this meta-analysis are multi-fold. First, it highlights the need for continued research elucidating the interplay between specific pollutant sources and mixtures present in particular locations, weather patterns dispersing/concentrating ambient contamination, and genetic factors affecting individual susceptibilities, all of which govern real-world exposures and COVID-19 risks. This can guide targeted risk communication and preventative interventions for those facing the highest level of threat. Second, these findings underscore the urgent necessity of implementing air pollution control policies and environmental public health measures worldwide to mitigate the synergetic effects of pollution and respiratory diseases. As countries continue reopening their economies, pollution levels return to traditional norms after transient declines during peak COVID-19 lockdowns in 2020. However, model estimates indicate that just a small sustained reduction in fossil fuel-derived PM2.5 in urban regions would appreciably decrease future COVID-19 death toll in addition to lowering background morbidity and mortality from non-communicable diseases.
Strategies such as transitioning energy production towards renewable and low-emission sources, enhancing industrial and vehicular emission standards, promoting alternative green transportation through improved infrastructure for walking, cycling, and public transit, increasing low-emission zones, implementing car restriction policies in polluted city centers, and augmenting urban greenspaces can effectively mitigate exposures and protect vulnerable populations from the synergistic effects of pollution and respiratory infections. For developing nations that still lack extensive air monitoring systems, rapidly deployable low-cost sensor networks hold promise for gathering local data to guide interventions. Critically, international awareness of the interconnected threats of air pollution and pandemic respiratory diseases must inform the development of integrated health, energy, and climate policies targeting sustainable development and pollution reduction. The environmental determinants of communicable and non-communicable diseases worldwide are inexorably linked. Therefore, promoting climate change mitigation through decarbonization offers vital co-benefits for immediate public health alongside long-term ecological stability. The devastating impacts of the COVID-19 pandemic and the specter of future viral threats compel reconsideration of humanity’s relationship with nature.
4. Conclusion
This systematic review and meta-analysis provides compelling evidence for a significant association between exposure to air pollutants, specifically NO2, PM2.5, and PM10, and COVID-19 mortality. The findings indicate that both long-term and short-term exposure to these pollutants increase the risk of death from COVID-19, with the strongest association observed for PM2.5. Furthermore, the study highlights that without the implementation of appropriate policies, the adverse effects of air pollution, a global challenge, could exacerbate health problems. Therefore, it is crucial to design and implement strategies to manage and mitigate the risks associated with air pollution across various dimensions. Adopting integrated approaches is essential, as climate change contributes to the deterioration of numerous natural and human systems.
Acknowledgments
The authors would like to acknowledge Hamadan University of Medical Sciences for supporting this research (Project Number: 140105043255).
Authors’ Contribution
Conceptualization: Younes Mohammadi.
Data curation: Marzieh Fattahi-Darghlou.
Formal analysis: Marzieh Fattahi-Darghlou.
Funding acquisition: Younes Mohammadi.
Investigation: Hoda Arabzadeh.
Methodology: Younes Mohammadi.
Project administration: Marzieh Fattahi-Darghlou.
Resources: Younes Mohammadi.
Software: Marzieh Fattahi-Darghlou.
Supervision: Younes Mohammadi.
Validation:Younes Mohammadi.
Visualization: Hoda Arabzadeh.
Writing–original draft: Hoda Arabzadeh- Marzieh Fattahi-Darghlou.
Writing–review & editing: Hoda Arabzadeh- Marzieh Fattahi-Darghlou-Younes Mohammadi.
Competing Interests
The authors declared no conflict of interests regarding this research.
Ethical Approval
This research was confirmed by the Ethics Committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1401.314).
Funding
This research was financially supported by Hamadan University of Medical Sciences (Project Number: 140105043255).
References
- Maleki Roveshti M, Khajehnasiri F, Akhlaghi Pirposhteh E, Amanat N, Salehi Sahlabadi A, Vatani J. A systematic review on the climate and ecosystem change associated with the COVID-19 epidemic: global challenges. Avicenna J Environ Health Eng 2022; 9(2):117-23. doi: 10.34172/ajehe.2022.4209 [Crossref] [ Google Scholar]
- Worldometer. Coronavirus. Available from: https://www.worldometers.info/coronavirus/. Updated August 5, 2022.
- Ho CC, Hung SC, Ho WC. Effects of short- and long-term exposure to atmospheric pollution on COVID-19 risk and fatality: analysis of the first epidemic wave in northern Italy. Environ Res 2021; 199:111293. doi: 10.1016/j.envres.2021.111293 [Crossref] [ Google Scholar]
- Filippini T, Rothman KJ, Cocchio S, Narne E, Mantoan D, Saia M. Associations between mortality from COVID-19 in two Italian regions and outdoor air pollution as assessed through tropospheric nitrogen dioxide. Sci Total Environ 2021; 760:143355. doi: 10.1016/j.scitotenv.2020.143355 [Crossref] [ Google Scholar]
- Khan YA. Risk of mortality due to COVID-19 and air pollution in Pakistan. Environ Sci Pollut Res Int 2022; 29(2):2063-72. doi: 10.1007/s11356-021-15654-z [Crossref] [ Google Scholar]
- López-Feldman A, Heres D, Marquez-Padilla F. Air pollution exposure and COVID-19: a look at mortality in Mexico City using individual-level data. Sci Total Environ 2021; 756:143929. doi: 10.1016/j.scitotenv.2020.143929 [Crossref] [ Google Scholar]
- Karan A, Ali K, Teelucksingh S, Sakhamuri S. The impact of air pollution on the incidence and mortality of COVID-19. Glob Health Res Policy 2020; 5:39. doi: 10.1186/s41256-020-00167-y [Crossref] [ Google Scholar]
- Karuppasamy MB, Seshachalam S, Natesan U, Ayyamperumal R, Karuppannan S, Gopalakrishnan G. Air pollution improvement and mortality rate during COVID-19 pandemic in India: global intersectional study. Air Qual Atmos Health 2020; 13(11):1375-84. doi: 10.1007/s11869-020-00892-w [Crossref] [ Google Scholar]
- Wu X, Nethery RC, Sabath MB, Braun D, Dominici F. Exposure to air pollution and COVID-19 mortality in the United States: a nationwide cross-sectional study. medRxiv [Preprint]. April 27, 2020. Available from: https://www.medrxiv.org/content/10.1101/2020.04.05.20054502v2.
- Semczuk-Kaczmarek K, Rys-Czaporowska A, Sierdzinski J, Kaczmarek LD, Szymanski FM, Platek AE. Association between air pollution and COVID-19 mortality and morbidity. Intern Emerg Med 2022; 17(2):467-73. doi: 10.1007/s11739-021-02834-5 [Crossref] [ Google Scholar]
- Dettori M, Deiana G, Balletto G, Borruso G, Murgante B, Arghittu A. Air pollutants and risk of death due to COVID-19 in Italy. Environ Res 2021; 192:110459. doi: 10.1016/j.envres.2020.110459 [Crossref] [ Google Scholar]
- Konstantinoudis G, Padellini T, Bennett J, Davies B, Ezzati M, Blangiardo M. Long-term exposure to air-pollution and COVID-19 mortality in England: a hierarchical spatial analysis. Environ Int 2021; 146:106316. doi: 10.1016/j.envint.2020.106316 [Crossref] [ Google Scholar]
- Barnett-Itzhaki Z, Levi A. Effects of chronic exposure to ambient air pollutants on COVID-19 morbidity and mortality - a lesson from OECD countries. Environ Res 2021; 195:110723. doi: 10.1016/j.envres.2021.110723 [Crossref] [ Google Scholar]
- Coker ES, Cavalli L, Fabrizi E, Guastella G, Lippo E, Parisi ML. The effects of air pollution on COVID-19 related mortality in Northern Italy. Environ Resour Econ (Dordr) 2020; 76(4):611-34. doi: 10.1007/s10640-020-00486-1 [Crossref] [ Google Scholar]
- Marquès M, Rovira J, Nadal M, Domingo JL. Effects of air pollution on the potential transmission and mortality of COVID-19: a preliminary case-study in Tarragona province (Catalonia, Spain). Environ Res 2021; 192:110315. doi: 10.1016/j.envres.2020.110315 [Crossref] [ Google Scholar]
- Valdés Salgado M, Smith P, Opazo MA, Huneeus N. Long-term exposure to fine and coarse particulate matter and COVID-19 incidence and mortality rate in Chile during 2020. Int J Environ Res Public Health 2021; 18(14):7409. doi: 10.3390/ijerph18147409 [Crossref] [ Google Scholar]
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015; 4(1):1. doi: 10.1186/2046-4053-4-1 [Crossref] [ Google Scholar]
- Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 2010; 25(9):603-5. doi: 10.1007/s10654-010-9491-z [Crossref] [ Google Scholar]
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). Cochrane, 2024. Available from: www.training.cochrane.org/handbook.
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327(7414):557-60. doi: 10.1136/bmj.327.7414.557 [Crossref] [ Google Scholar]
- Sterne JA, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol 2000; 53(11):1119-29. doi: 10.1016/s0895-4356(00)00242-0 [Crossref] [ Google Scholar]
- Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994; 50(4):1088-101. [ Google Scholar]
- Duval S, Tweedie R. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. J Am Stat Assoc 2000; 95(449):89-98. doi: 10.1080/01621459.2000.10473905 [Crossref] [ Google Scholar]
- Aloisi V, Gatto A, Accarino G, Donato F, Aloisio G. The effect of known and unknown confounders on the relationship between air pollution and COVID-19 mortality in Italy: a sensitivity analysis of an ecological study based on the E-value. Environ Res 2022; 207:112131. doi: 10.1016/j.envres.2021.112131 [Crossref] [ Google Scholar]
- Dales R, Blanco-Vidal C, Romero-Meza R, Schoen S, Lukina A, Cakmak S. The association between air pollution and COVID-19 related mortality in Santiago, Chile: a daily time series analysis. Environ Res 2021; 198:111284. doi: 10.1016/j.envres.2021.111284 [Crossref] [ Google Scholar]
- De Angelis E, Renzetti S, Volta M, Donato F, Calza S, Placidi D. COVID-19 incidence and mortality in Lombardy, Italy: an ecological study on the role of air pollution, meteorological factors, demographic and socioeconomic variables. Environ Res 2021; 195:110777. doi: 10.1016/j.envres.2021.110777 [Crossref] [ Google Scholar]
- Garcia E, Marian B, Chen Z, Li K, Lurmann F, Gilliland F. Long-term air pollution and COVID-19 mortality rates in California: findings from the spring/summer and winter surges of COVID-19. Environ Pollut 2022; 292(Pt B):118396. doi: 10.1016/j.envpol.2021.118396 [Crossref] [ Google Scholar]
- Hadei M, Hopke PK, Shahsavani A, Raeisi A, Jafari AJ, Yarahmadi M. Effect of short-term exposure to air pollution on COVID-19 mortality and morbidity in Iranian cities. J Environ Health Sci Eng 2021; 19(2):1807-16. doi: 10.1007/s40201-021-00736-4 [Crossref] [ Google Scholar]
- Hu H, Zheng Y, Wen X, Smith SS, Nizomov J, Fishe J. An external exposome-wide association study of COVID-19 mortality in the United States. Sci Total Environ 2021; 768:144832. doi: 10.1016/j.scitotenv.2020.144832 [Crossref] [ Google Scholar]
- Meo SA, Abukhalaf AA, Alessa OM, Alarifi AS, Sami W, Klonoff DC. Effect of environmental pollutants PM25, CO, NO2, and O3 on the incidence and mortality of SARS-CoV-2 infection in five regions of the USA. Int J Environ Res Public Health 2021; 18(15):7810. doi: 10.3390/ijerph18157810 [Crossref] [ Google Scholar]
- Petroni M, Hill D, Younes L, Barkman L, Howard S, Howell IB. Hazardous air pollutant exposure as a contributing factor to COVID-19 mortality in the United States. Environ Res Lett 2020; 15(9):0940a9. doi: 10.1088/1748-9326/abaf86 [Crossref] [ Google Scholar]
- Sanchez-Piedra C, Cruz-Cruz C, Gamiño-Arroyo AE, Prado-Galbarro FJ. Effects of air pollution and climatology on COVID-19 mortality in Spain. Air Qual Atmos Health 2021; 14(11):1869-75. doi: 10.1007/s11869-021-01062-2 [Crossref] [ Google Scholar]
- Tian F, Liu X, Chao Q, Qian ZM, Zhang S, Qi L. Ambient air pollution and low temperature associated with case fatality of COVID-19: a nationwide retrospective cohort study in China. Innovation (Camb) 2021; 2(3):100139. doi: 10.1016/j.xinn.2021.100139 [Crossref] [ Google Scholar]
- Xing YF, Xu YH, Shi MH, Lian YX. The impact of PM25 on the human respiratory system. J Thorac Dis 2016; 8(1):E69-74. doi: 10.3978/j.issn.2072-1439.2016.01.19 [Crossref] [ Google Scholar]
- Wang Q, Liu S. The effects and pathogenesis of PM25 and its components on chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis 2023; 18:493-506. doi: 10.2147/copd.S402122 [Crossref] [ Google Scholar]
- Islam MS, Saha SC, Gemci T, Yang IA, Sauret E, Gu YT. Polydisperse microparticle transport and deposition to the terminal bronchioles in a heterogeneous vasculature tree. Sci Rep 2018; 8(1):16387. doi: 10.1038/s41598-018-34804-x [Crossref] [ Google Scholar]
- Dondi A, Carbone C, Manieri E, Zama D, Del Bono C, Betti L. Outdoor air pollution and childhood respiratory disease: the role of oxidative stress. Int J Mol Sci 2023; 24(5):4345. doi: 10.3390/ijms24054345 [Crossref] [ Google Scholar]
- Sarvi F, Nadali A, Khodadost M, Kharghani Moghaddam M, Sadeghifar M. Application of poisson hidden markov model to predict number of PM25 exceedance days in Tehran during 2016-2017. Avicenna J Environ Health Eng 2017; 4(1):58031. doi: 10.5812/ajehe.58031 [Crossref] [ Google Scholar]
- Pardo M, Qiu X, Zimmermann R, Rudich Y. Particulate matter toxicity is Nrf2 and mitochondria dependent: the roles of metals and polycyclic aromatic hydrocarbons. Chem Res Toxicol 2020; 33(5):1110-20. doi: 10.1021/acs.chemrestox.0c00007 [Crossref] [ Google Scholar]
- Shen J, Taghvaee S, La C, Oroumiyeh F, Liu J, Jerrett M. Aerosol oxidative potential in the greater Los Angeles area: source apportionment and associations with socioeconomic position. Environ Sci Technol 2022; 56(24):17795-804. doi: 10.1021/acs.est.2c02788 [Crossref] [ Google Scholar]
- Kelly FJ, Fussell JC. Role of oxidative stress in cardiovascular disease outcomes following exposure to ambient air pollution. Free Radic Biol Med 2017; 110:345-67. doi: 10.1016/j.freeradbiomed.2017.06.019 [Crossref] [ Google Scholar]
- Ali N, Islam F. The effects of air pollution on COVID-19 infection and mortality-a review on recent evidence. Front Public Health 2020; 8:580057. doi: 10.3389/fpubh.2020.580057 [Crossref] [ Google Scholar]
- Li D, Wang X, Liao Y, Wang S, Shan J, Ji J. Insights gained into the treatment of COVID-19 by pulmonary surfactant and its components. Front Immunol 2022; 13:842453. doi: 10.3389/fimmu.2022.842453 [Crossref] [ Google Scholar]
- Ratajczak MZ, Bujko K, Ciechanowicz A, Sielatycka K, Cymer M, Marlicz W. SARS-CoV-2 entry receptor ACE2 is expressed on very small CD45(-) precursors of hematopoietic and endothelial cells and in response to virus spike protein activates the Nlrp3 inflammasome. Stem Cell Rev Rep 2021; 17(1):266-77. doi: 10.1007/s12015-020-10010-z [Crossref] [ Google Scholar]
- Borro M, Di Girolamo P, Gentile G, De Luca O, Preissner R, Marcolongo A. Evidence-based considerations exploring relations between SARS-CoV-2 pandemic and air pollution: involvement of PM25-mediated up-regulation of the viral receptor ACE-2. Int J Environ Res Public Health 2020; 17(15):5573. doi: 10.3390/ijerph17155573 [Crossref] [ Google Scholar]
- Frontera A, Cianfanelli L, Vlachos K, Landoni G, Cremona G. Severe air pollution links to higher mortality in COVID-19 patients: the “double-hit” hypothesis. J Infect 2020; 81(2):255-9. doi: 10.1016/j.jinf.2020.05.031 [Crossref] [ Google Scholar]
- Ko UW, Kyung SY. Adverse effects of air pollution on pulmonary diseases. Tuberc Respir Dis (Seoul) 2022; 85(4):313-9. doi: 10.4046/trd.2022.0116 [Crossref] [ Google Scholar]
- Carroquino MJ, Posada M, Landrigan PJ. Environmental toxicology: children at risk. In: Laws EA, ed. Environmental Toxicology: Selected Entries from the Encyclopedia of Sustainability Science and Technology. New York, NY: Springer; 2013. p. 239-91. doi: 10.1007/978-1-4614-5764-0_11.
- Wu K, Zhang Y, Austin SR, Yin-Declue H, Byers DE, Crouch EC. Lung remodeling regions in long-term coronavirus disease 2019 feature basal epithelial cell reprogramming. Am J Pathol 2023; 193(6):680-9. doi: 10.1016/j.ajpath.2023.02.005 [Crossref] [ Google Scholar]
- Brągoszewska E, Mainka A. Impact of different air pollutants (PM10, PM25, NO2, and bacterial aerosols) on COVID-19 cases in Gliwice, Southern Poland. Int J Environ Res Public Health 2022; 19(21):14181. doi: 10.3390/ijerph192114181 [Crossref] [ Google Scholar]
- Kwon SO, Hong SH, Han YJ, Bak SH, Kim J, Lee MK. Long-term exposure to PM10 and NO2 in relation to lung function and imaging phenotypes in a COPD cohort. Respir Res 2020; 21(1):247. doi: 10.1186/s12931-020-01514-w [Crossref] [ Google Scholar]
- Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis 2017; 12:2891-908. doi: 10.2147/copd.S139470 [Crossref] [ Google Scholar]
- Hamanaka RB, Mutlu GM. Particulate matter air pollution: effects on the cardiovascular system. Front Endocrinol (Lausanne) 2018; 9:680. doi: 10.3389/fendo.2018.00680 [Crossref] [ Google Scholar]
- Kilic H, Arguder E, Karalezli A, Unsal E, Guner R, Kayaslan B. Effect of chronic lung diseases on mortality of prevariant COVID-19 pneumonia patients. Front Med (Lausanne) 2022; 9:957598. doi: 10.3389/fmed.2022.957598 [Crossref] [ Google Scholar]
- Li X, Zhong X, Wang Y, Zeng X, Luo T, Liu Q. Clinical determinants of the severity of COVID-19: a systematic review and meta-analysis. PLoS One 2021; 16(5):e0250602. doi: 10.1371/journal.pone.0250602 [Crossref] [ Google Scholar]
- Alqahtani JS, Oyelade T, Aldhahir AM, Alghamdi SM, Almehmadi M, Alqahtani AS. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis. PLoS One 2020; 15(5):e0233147. doi: 10.1371/journal.pone.0233147 [Crossref] [ Google Scholar]
- Katoto P, Brand AS, Bakan B, Obadia PM, Kuhangana C, Kayembe-Kitenge T. Acute and chronic exposure to air pollution in relation with incidence, prevalence, severity and mortality of COVID-19: a rapid systematic review. Environ Health 2021; 20(1):41. doi: 10.1186/s12940-021-00714-1 [Crossref] [ Google Scholar]
- Badida P, Krishnamurthy A, Jayaprakash J. Meta-analysis of health effects of ambient air pollution exposure in low- and middle-income countries. Environ Res 2023; 216(Pt 4):114604. doi: 10.1016/j.envres.2022.114604 [Crossref] [ Google Scholar]