Avicenna J Environ Health Eng. 10(2):103-109.
doi: 10.34172/ajehe.5395
Original Article
The Correlation of Family Access to Clear Water with Diarrheal Disease Incidence in the Working Area of the Sumbersari Health Center, Jember Regency
Hanifah Rahmawati 1  , Tantut Susanto 2, * , Fahruddin Kurdi 2 , Fitrio Deviantony 3 , Wahyuni Fauziah 4
, Tantut Susanto 2, * , Fahruddin Kurdi 2 , Fitrio Deviantony 3 , Wahyuni Fauziah 4
Author information:
1Undergraduate Nursing Program, Faculty of Nursing, University of Jember, Indonesia
2Department of Community, Family, and Geriatric Nursing, Faculty of Nursing, University of Jember, Indonesia
3Department of Mental Health Nursing, Faculty of Nursing, University of Jember, Indonesia
4Neurology Department, Dr. H Koesnadi Regional Hospital of Bondowoso, East Java, Indonesia
Abstract
Diarrhea is one of the digestive problems characterized by a decrease in fluid followed by a loss of electrolytes in the body; therefore, it requires further treatment so as not to cause more severe problems. The incidence of diarrheal disease can be influenced by optimal or inadequate access to clear water. This study aims to determine the relationship between family access to clear water and the incidence of diarrheal diseases in the working area of the Sumbersari Health Center, Jember Regency. This study was a non-experimental analytic research with a case-control design. The sample consisted of 140 participants in the case group and 140 participants in the control group, selected by the simple random sampling technique. Participants who met the inclusion and exclusion criteria were recruited into the study. Data collection tools included a demographic characteristics questionnaire, a questionnaire on clear water access, and a questionnaire about diarrhea disease incidence. Data analysis was performed using the Chi-square test (P<0.05). The results showed that most of the respondents had optimal access to clear water (31.1% in the case group and 42.9% in the control group). Diarrhea sufferers were mostly in the early adult category (21.8%). Then, there is a significant relationship between family access to clear water and the incidence of diarrheal disease in the Sumbersari Public Health Center, Jember Regency (P<0.001; OR: 0.274).
Keywords: Clear water access, Diarrhea, Family, Jember Regency,
Copyright and License Information
© 2023 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Rahmawati H, Susanto T, Kurdi F, Deviantony F, Fauziah W. The correlation of family access to clear water with diarrheal disease incidence in the working area of the Sumbersari Health Center, Jember Regency. Avicenna J Environ Health Eng. 2023; 10(2):103-109. doi:10.34172/ajehe.5395
1. Introduction
Diarrhea is one of the health problems that hit various countries. According to data from the World Health Organization (WHO), 2 billion cases of diarrhea occur worldwide, and 1.8 billion people die each year due to it (1,2). According to the Ministry of Health of the Republic of Indonesia, there were 10 diarrheal cases in 2018 that occurred in 8 provinces of Indonesia, 756 cases and 36 deaths (3). Jember is one of the major contributors to diarrhea. Based on data from the Health Profile of Jember District in 2020, 20086 cases of diarrhea occurred (4). According to data from the Jember District Health Office in 2022, the Sumbersari Health Center work area has the highest incidence of diarrheal disease in the Jember Regency, with 2414 cases (5).
Restuti and Fitri also reported that the Sumbersari Health Center is the major contributor to the incidence of diarrhea among toddlers, 1256 cases (5.5%) out of a total of 22 590 cases (6). Sumbersari Health Center is located in an urban area but has the highest incidence rate in Jember Regency. According to data from the Central Statistics Agency for 2019, urban areas have a higher percentage of access to proper sanitation than rural areas (93.32% vs. 78.61%) (7). Most residents in Jember Regency live in dense residential areas which tend to have poorly maintained environments and limited provision of basic infrastructure, including the availability of clear water and sanitation infrastructure (7). This means that people with access to proper sanitation (clear water facilities) should have a low incidence of diarrhea.
The Indonesian Nursing Diagnosis Standard defines diarrhea as defecation (disposal of feces) of soft and liquid stools that occur more than three times in one day (8). Cases of diarrhea can be caused by several factors, including the low level of access to clear water, food and drink contaminated with viruses and bacteria, behavioral factors such as the low frequency of washing hands before and after eating or defecating, and the unavailability of healthy latrines (9). The prevalence of diarrhea was found to be associated with several factors, including the level of knowledge, attitudes towards diarrhea, access to clear water, strategies to prevent diarrheal disease, and use of trash (10). Families who experience diarrheal disease can take some prevention and treatment steps. Preventive actions that families can do include breastfeeding toddlers, using clear water in all life activities, washing hands with soap and running water, and using healthy latrines, which can decrease the incidence of diarrheal diseases (11). Oral rehydration solution (ORS), breast milk (for patients < 2 years), and honey can also be used for the treatment of diarrhea (12).
Efforts to eradicate diarrheal diseases certainly require contributions from the family. According to Friedman et al, there are five family functions: affective, socialization, reproduction, economy, and care functions (13-15). The function of health care is a family function that has a large contribution to this study, considering that families have a significant share in meeting the needs to clothing, food, shelter, and health to be protected from various hazards (13). The family has a vital role as a provider of comfort and safety for the living environment, as stated in the Healthy Indonesia Program with a Family Approach, which is scheduled by the government (16). The role of a nurse in the family is to act as executor of promotive, preventive, curative, and rehabilitative efforts from one house to another regarding access to clear water so that the PIS-PK target can be adequately realized.
Based on the problems described above, this study aimed to analyze the relationship between family access to clear water and the incidence of diarrheal disease in the working area of the Sumbersari Health Center, Jember Regency.
2. Materials and Methods
This quantitative study used an observational analytic design with a case-control approach (data from December 2022 to February 2023). It was conducted in the working area of the Sumbersari Health Center, Jember Regency, East Java (Fig. 1). This case-control study aimed to identify the relationship between the two variables in the case and control groups and to study the extent to which risk factors trigger effects (17). The population of this study included people who were part of a family living in the working area of the Sumbersari Health Center, Jember Regency, 358 people (179 in the case group and 179 in the control group). The sample size was calculated using the case-control formula considering a confidence interval of 95%, significance level of Z1-α/2 = 1.96, the error rate of α = 0.05, P1 = 0.299, and P2 = 0.162. Finally, a total of 140 participants were included in the case group and 140 participants in the control group. The research sample was taken using the simple random sampling technique in Microsoft Excel. The respondents who met the inclusion and exclusion criteria were included in the study. The inclusion criteria for both the case and control groups were being part of a family living in the Sumbersari Health Center work area and using clear water daily. Respondents who were not willing to be part of the research sample were excluded from the study.
Demographic characteristics of the participants included home address, gender, age, education level, occupation of the head of the family, income, number of family members (in one house), type of primary source of clear water, the distance between clear water facilities and landfills and septic tanks, health promotion related to clear water facilities and diarrheal diseases, way of consuming drinking water, and practice of handwashing with soap. Access to clear water was determined with a questionnaire from the WHO, which was translated into Indonesian by Maryono (18,19). The questionnaire has three assessment indicators (quantity, distance, and time), listed with further details in Table 1.
Table 1.
Indicators of Access to Clear Water in the Household
|
Quantity
|
Distance
|
Time
|
Mark
|
| 5-19 liter/person/day |
> 1000 meter |
> 30 minute |
0 |
| 20-49 liter/person/day |
100-1000 meter |
5-30 minute |
1 |
| 50-99 liter/person/day |
< 100 meter |
< 5 minutes (1 house, 1 faucet) |
2 |
| > 100 liter/person/day |
1 house > 1 faucet |
1 house > 1 faucet |
3 |
Source: Howard and Bartram (2003) in (Maryono, 2007).
The access to clear water in households was categorized into 4 levels, including no access, basic access, intermediate access, and optimal access (Table 2).
Table 2.
Level of Access to Clear Water in the Household
|
Level
|
Total score
|
| No access |
0 |
| Basic access |
1-3 |
| Intermediate access |
0-8 |
| Optimal access |
7-9 |
Source: Howard and Bartram (2003) in (Maryono, 2007).
To facilitate data processing with the Chi-square test, the access to clear water was categorized into 2 levels, not optimal access to clear water with a score range of 0 to 6 and optimal access to clear water with a score range of 7 to 9. According to the Indonesian Nursing Diagnosis Standards, the incidence of diarrheal disease was determined based on 2 categories: diarrhea and no diarrhea (8). The participants were asked whether they had had bowel movements with soft and liquid stools > 3 times a day for the last 3 months.
The questionnaire on respondent characteristics and access to clear water uses primary data, while the questionnaire for diarrheal disease incidence uses secondary data from primary and auxiliary health centers. The researcher explained the objectives of the research to prospective respondents before collecting data. Respondents who wished to participate in the study were given informed consent and further information. Data collection was carried out directly by respondents/guardians of respondents who were met by researchers with the assistance of local midwives/nurses/cadres in March 2023. The research was approved by the Health Research Ethics Committee of the Faculty of Nursing, University of Jember (023/UN25.1.14/KEPK/2023).
The research data were then analyzed using IBM SPSS version 25.0. After processing, the data were presented as frequency tables and bar charts. Characteristics of the participants were displayed using a frequency table. At the same time, for the data on access to clear water and the incidence of diarrheal diseases, a combination of frequency tables and bar charts were used. Categorical data were presented in the form of frequency and percentage. Meanwhile, numerical data were presented using median and percentile (25-75). Bivariate analysis was carried out to determine the relationship between family access to clear water and the incidence of diarrheal disease in the Sumbersari Health Center, Jember Regency, using the chi-square test with a significance level of P < 0.05. Chi-square is suitable for ordinal or categorical variables where the data can be categorized into levels or categories. It is not suitable for continuous variables.
3. Results and Discussion
The characteristics of the respondents are presented in Table 3. Researchers used frequencies and percentages for presenting categorical data to make interpretation of the data easier. Meanwhile, the median was used in numerical data because the data were not normally distributed. The median age of the respondents was significantly higher in the control group, which was 37 years, compared to the case group, which had a median age of 20 years. A high proportion of home addresses in the case group belonged to Tegalboto area, with 70 respondents (25%). In contrast, a high proportion of respondents in the control group lived in Tegalgede and Antirogo areas, each with 70 respondents (25%). The frequency of female gender was significantly higher in the control group, 115 people (41.1%), compared to the case group with 78 people (27.9%). Based on the results, 41 people (14.6%) in the case group and 44 people (15.7%) in the control group had a high school education level, indicating that it was significantly more prevalent than other levels.
Table 3.
Characteristics of Respondents in the Working Area of the Sumbersari Health Center, Jember Regency (N = 280)
|
Characteristics of respondents
|
Group
|
|
Case (n=140)
|
Control (n=140)
|
|
|
Median(P25-P75)
|
Median (P25-P75)
|
| Age |
20 (6-33.75)
|
37 (28-52)
|
|
|
No.
|
%
|
No.
|
%
|
| Home address |
|
|
|
|
| Antirogo |
0 |
0 |
70 |
25 |
| Karangrejo |
35 |
12.5 |
0 |
0 |
| Tegalboto Sumbersari |
70 |
25 |
0 |
0 |
| Tegalgede |
0 |
0 |
70 |
25 |
| Wirolegi |
35 |
12.5 |
0 |
0 |
| Gender |
|
|
|
|
| Male |
62 |
22.1 |
25 |
8.9 |
| Female |
78 |
27.9 |
115 |
41.1 |
| Education level |
|
|
|
|
| No school |
30 |
10.7 |
9 |
3.2 |
| Kindergarten |
20 |
7.1 |
1 |
0.4 |
| Elementary school |
20 |
7.1 |
42 |
15 |
| Junior high school |
19 |
6.8 |
24 |
8.6 |
| Senior high school |
41 |
14.6 |
44 |
15.7 |
| Diploma/bachelor's degree/master's degree/Ph.D. |
10 |
3.6 |
20 |
7.1 |
| Occupation of the head of the family |
|
|
|
|
| Does not work |
1 |
0.4 |
12 |
4.3 |
| Housewife |
6 |
2.1 |
9 |
3.2 |
| Government employee |
32 |
11.4 |
15 |
5.4 |
| Farmer |
11 |
3.9 |
4 |
1.4 |
| Entrepreneur |
61 |
21.8 |
46 |
16.4 |
| Private sector employee |
20 |
7.1 |
20 |
7.1 |
| Construction laborers |
9 |
3.2 |
34 |
12.1 |
| Income of the head of the family |
|
|
|
|
| < City minimum wage |
75 |
26.8 |
101 |
36.1 |
| > City minimum wage |
65 |
23.2 |
39 |
13.9 |
| Number of family members |
|
|
|
|
| 1 person |
0 |
0 |
0 |
0 |
| 2 persons |
37 |
13.2 |
20 |
7.1 |
| 3 people |
46 |
16.4 |
47 |
16.8 |
| 4 people |
41 |
14.6 |
41 |
14.6 |
| 5 people |
6 |
2.1 |
23 |
8.2 |
| 6 people |
10 |
3.6 |
5 |
1.8 |
| 7 people |
0 |
0 |
4 |
1.4 |
| Primary source of clear water |
|
|
|
|
| Well water |
81 |
28.9 |
26 |
9.3 |
| Local water company |
59 |
21.1 |
114 |
40.7 |
| Location of clear water facilities with landfills and septic tanks ( > 10 m) |
|
|
|
|
| Yes |
125 |
44.6 |
115 |
41.1 |
| No |
15 |
5.4 |
25 |
8.9 |
| Health promotion gains |
|
|
|
|
| Yes, I have. |
108 |
38.6 |
128 |
45.7 |
| Never |
32 |
11.4 |
12 |
4.3 |
| How to consume drinking water |
|
|
|
|
| Boiling water |
61 |
21.8 |
76 |
27.1 |
| Water gallon |
79 |
28.2 |
61 |
21.8 |
| Filtering water |
0 |
0 |
3 |
1.1 |
| Knowledge of hand washing |
|
|
|
|
| Yes, I have. |
140 |
50 |
137 |
48.9 |
| Still waiting |
0 |
0 |
3 |
1.1 |
The frequency of working as an entrepreneur was significantly higher in the case group compared to the control group (61 respondents [21.8%] vs. 46 respondents [16.4%]). The frequency of income below the minimum wage was significantly higher in the control group, 101 respondents (36.1%), compared to the case group, with 75 respondents (26.8%). The majority of families in the control and case groups had 3 members (47 respondents [16.8%] vs. 46 respondents [16.4%]).
Well water had a significantly higher frequency in the case group, 81 respondents (28.9%), compared to the control group, which amounted to 26 respondents (9.3%). The distance between the clear water facilities and landfill site and septic tanks for the majority of the respondents in the two groups was more than 10 m, 125 respondents (44.6%) in the case group and 115 respondents (41.1%) in the control group. The number of participants who answered “yes” to health promotion gains was significantly higher in the control group compared to the case group, 128 respondents (45.7%) vs. 108 respondents (38.6%).
The proportion of drinking water in gallons or bottles was significantly higher in the case group, 79 respondents (28.2%), compared to the control group, which amounted to 61 respondents (21.8%). The majority already knew how to wash hands in the two groups of respondents, 140 respondents (50%) in the case group and 137 respondents (48.9%) in the control group.
Based on the data obtained from each indicator of access to clear water, the results showed that some groups had optimal access to clear water and some did not. The number of people who did not have optimal access to clear water was significantly higher in the case group compared to the control group, 53 respondents (18.9%) vs. 20 respondents (7.1%). Further data are shown in Fig. 2.
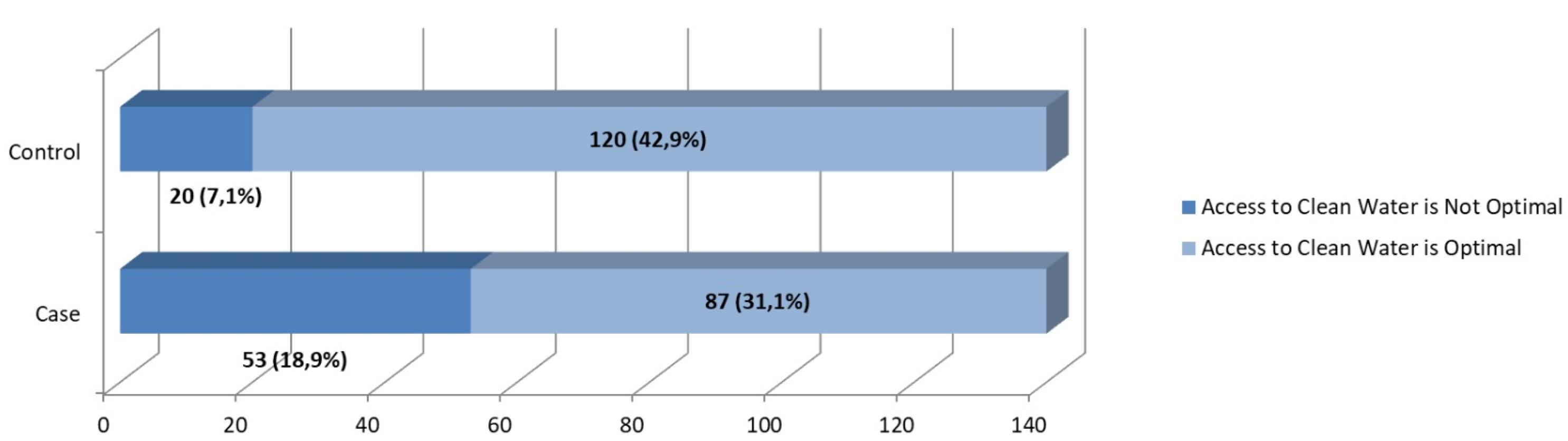
Fig. 2.
Access to Clear Water Indicators in the Case and Control Groups
.
Access to Clear Water Indicators in the Case and Control Groups
Various age groups experienced diarrhea. However, according to the Ministry of Health of the Republic of Indonesia, the majority of respondents with diarrhea in the working area of Sumbersari District Health Center were in the early adult category (26–35 years). A further explanation of this finding is presented in Fig. 3.
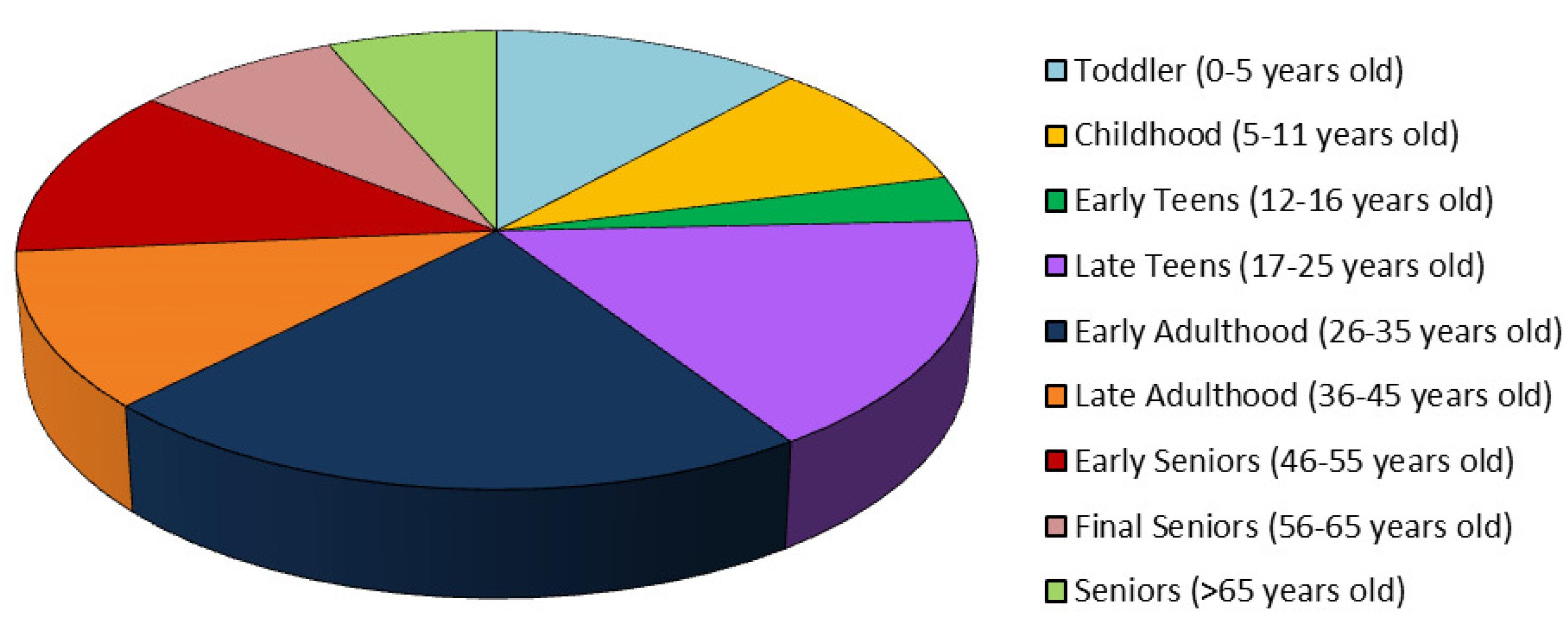
Fig. 3.
The Incidence of Diarrhea in the Working Area of the Sumbersari Health Center, Jember Regency
.
The Incidence of Diarrhea in the Working Area of the Sumbersari Health Center, Jember Regency
The results of chi-square test (Table 4) show that there is a relationship between family access to clear water and the incidence of diarrheal disease in the Sumbersari Health Center work area (P < 0.001, OR: 0.274).
Table 4.
Relationship between Family Access to Clear Water and Diarrhea in the Working Area of the Sumbersari Health Center (N = 280)
|
Clear Water Access
|
Diarrheal Disease Incidence
|
χ2
|
OR
(95% CI)
|
P
Value
|
|
Case
|
Control
|
|
No.
|
%
|
No.
|
%
|
| Not optimal access |
53 |
37.9 |
20 |
14.3 |
20.179 |
0.274
(0.153-0.490) |
< 0.001 |
| Optimal access |
87 |
62.1 |
120 |
85.7 |
| Total |
140 |
100 |
140 |
100 |
OR: odds ratio, CI: confidence interval.
The results of this study indicated significant differences between the two groups in family access to clear water in the working area of the Sumbersari Health Center, Jember Regency. This is because the case and control families have various levels of access to clear water, ranging from optimal (case: 31.1%; control: 42.9%) to not optimal (case: 18.9%; control: 7.1%). Access to clear water is optimal; in this case, the majority have a quantity of clear water > 100 liters per person per day, and each house has > 1 water faucet, so the distance for taking it is not far, and the collection time is not long (20). However, access to clear water could be more optimal, judged by the lack or limitations of clear water facilities in the neighborhood (21). Therefore, families need to optimize access to clear water facilities such as healthy water and Perusahaan Daerah Air Minum (PDAM) so that their daily needs can be adequately met (4).
The results showed that diarrheal disease in the working area of the Sumbersari Health Center was experienced by people of various ages, with the majority being in the early adult group. This is due to the difference in the education level ( < junior high school: 35.7%) of the patients; therefore, preventive measures against diarrheal diseases have not been appropriately implemented. Individuals with low education levels tend to have minimal preventive efforts, so their health status needs to be improved (22). Higher education gives a person broad insight and an excellent orientation toward prevention (23). Therefore, every family member needs to increase his/her knowledge, which is obtained through health promotion provided by nurses, so that the incidence of diarrheal diseases can be avoided.
This study concludes that there is a relationship between family access to clear water and the incidence of diarrheal disease in the working area of the Sumbersari Health Center, Jember Regency. This is because most of the respondent’s families in the case group (21.1%) and control group (40.7%) already have access to clear water facilities (PDAM). The availability of adequate clear water facilities, in the form of PDAM water, can be a preventive factor while reducing the risk of diarrheal disease (24). Clear water facilities can improve the health status of families, considering that families with inadequate clear water facilities have 5 times greater risk of experiencing diarrhea (22). According to Florence Nightingale’s environmental theory, the availability of clear water, pure air, efficient drainage, cleanliness, and adequate light are the essential elements of the physical environment that need to be provided so that a person’s health status remains optimal (25). Therefore, families need to improve and maintain access to clear water facilities and pay attention to risk factors for diarrheal disease to avoid the related health problems. The results of this research can have an impact on regional health regulations, inspiring officials to fund projects and infrastructure that guarantee Jember Regency families have access to clear water. Effective preventive activities include community outreach initiatives, education campaigns, and water treatment facilities.
4. Conclusion
Based on the results, it can be concluded that there is a relationship between family access to clear water and the incidence of diarrheal disease in theworking area of the Sumbersari Health Center, Jember Regency.
Acknowledgments
The authors would like to acknowledge the Center of Agronursing for Community, Family and Elderly Health Studies, Department of Community, Family, and Geriatric Nursing, Faculty of Nursing, University of Jember for their contributions.
Authors’ Contribution
Conceptualization: Hanifah Rahmawati, Tantut Susanto, Fahruddin Kurdi.
Data curation: Hanifah Rahmawati, Tantut Susanto, Fahruddin Kurdi.
Formal analysis: Hanifah Rahmawati, Tantut Susanto, Fahruddin Kurdi.
Funding acquisition: Tantut Susanto.
Investigation: Hanifah Rahmawati, Fahruddin Kurdi.
Methodology: Hanifah Rahmawati, Tantut Susanto, Fahruddin Kurdi.
Project administration: Hanifah Rahmawati, Tantut Susanto.
Resources: Hanifah Rahmawati, Fahruddin Kurdi, Fitrio Deviantony.
Software: Hanifah Rahmawati, Fahruddin Kurdi, Fitrio Deviantony.
Supervision: Tantut Susanto, Fahruddin Kurdi.
Validation: Tantut Susanto, Fahruddin Kurdi, Wahyuni Fauziah.
Visualization: Tantut Susanto, Fahruddin Kurdi.
Writing–original draft: Hanifah Rahmawati, Tantut Susanto, Fahruddin Kurdi, Fitrio Deviantony.
Writing–review & editing: Tantut Susanto, Fahruddin Kurdi, Fitrio Deviantony, Wahyuni Fauziah.
Competing Interests
The authors declare no conflict of interests.
References
- Dharmayanti I, Tjandrarini DH. Peran lingkungan dan individu terhadap masalah diare di pulau jawa dan bali. Jurnal Ekologi Kesehatan 2020; 19(2):84-93. doi: 10.22435/jek.v19i2.3192 [Crossref] [ Google Scholar]
- Siregar S, Batubara NS. Faktor-faktor yang Mempengaruhi Kejadian Penyakit Diare di Desa Hutanopan Kecamatan Halongonan Kabupaten Padang Lawas Utara Tahun 2018. Indonesian Health Scientific Journal 2019; 4(1):26-34. [ Google Scholar]
- Kementerian Kesehatan. Profil Kesehatan Indonesia Tahun 2018. Jakarta: Kementerian Kesehatan; 2018.
- Javanmardi Z, Alighadri M, Parastar S, Sadeghi T. Effects of the municipal solid waste landfill on the quality of water resources in Khalkhal: a case study. Avicenna J Environ Health Eng 2022; 9(1):25-34. doi: 10.34172/ajehe.2022.04 [Crossref] [ Google Scholar]
- Jember District Health Profile. Profil Kesehatan Kabupaten Jember 2020. Jember: Dinas Kesehatan Kabupaten Jember; 2020.
- Jember District Health Office. Data Kejadian Diare Kabupaten Jember 2022. Jember District Health Office; 2022.
- Restuti AN, Fitri YA. Hubungan antara tingkat asupan vitamin A, Zinc, dan Polyunsaturated Fatty Acid (PUFA) dengan kejadian diare balita. Indones J Hum Nutr 2019; 6(1):32-40. doi: 10.21776/ub.ijhn.2019.006.01.4 [Crossref] [ Google Scholar]
- Central Statistics Agency. Persentase Rumah Tangga yang Memiliki Akses terhadap Sanitasi Layak. BPS East Java; 2019.
- Persatuan Perawat Nasional Indonesia (PPNI). Standar Diagnosis Keperawatan Indonesia: Definisi dan Indikator Diagnostik Edisi 1. Jakarta: PPNI; 2016.
- Melvani RP, Zulkifli H, Faizal M. Analisis faktor yang berhubungan dengan kejadian diare balita di Kelurahan Karyajaya Kota Palembang. JUMANTIK (Jurnal Ilmiah Penelitian Kesehatan) 2019; 4(1):57-68. doi: 10.30829/jumantik.v4i1.4052 [Crossref] [ Google Scholar]
- Prawati DD, Haqi DN. Faktor yang mempengaruhi kejadian diare di Tambak Sari, Kota Surabaya. Jurnal Promkes 2019; 7(1):34-45. doi: 10.20473/jpk.V7.I1.2019.34-45 [Crossref] [ Google Scholar]
- Ariyanto A, Fatmawati TY. Edukasi Pencegahan Diare Pada Anak di Kelompok Dasawisma Kelurahan Kenali Asam Bawah. Jurnal Salam Sehat Masyarakat 2021; 2(2):13-8. doi: 10.22437/jssm.v2i2.13611 [Crossref] [ Google Scholar]
- Sari RS, Solihat LL, Febriyana L, Mardianti M, Sari MP, Mirqotussyifa M. Meningkatkan Pengetahuan Mengenai Penanganan Diare Pada Anak Melalui Penyuluhan Kesehatan. Jurnal Pengabdian Masyarakat Berkemajuan 2021; 4(2):70-3. [ Google Scholar]
- Friedman MM, Bowden VR, Jones EG. Buku Ajar Keperawatan Keluarga: Riset, Teori, dan Praktek. Jakarta: EGC Medical Publisher; 2010.
- Pattiruhu IC, Rompas S, Simak V. Fungsi afektif keluarga dan fungsi sosialisasi keluarga dengan perilaku seksual remaja. Jurnal Keperawatan 2019; 7(2):1-9. doi: 10.35790/jkp.v7i2.24464 [Crossref] [ Google Scholar]
- Susanto T. Keperawatan Keluarga: Aplikasi Teori Pada Praktik Asuhan. Jakarta: Trans Info Media; 2021.
- Kementerian Kesehatan RI. Pedoman Umum: Program Indonesia Sehat dengan Pendekatan Keluarga. Jakarta: Kementerian Kesehatan RI; 2016.
- Yani RW. Riset Epidemiologi Bidang Kesehatan. Jember: UPT Percetakan dan Penerbitan Universitas Jember; 2019.
- Maryono M. Menilai Aksesibilitas Air Minum (Studi Kasus: Aksesibilitas Air Bersih Bagi Masyarakat Miskin Di Kota Semarang). Jurnal Presipitasi 2007; 3(2):86-92. [ Google Scholar]
- Howard G, Bartram J. Domestic Water Quantity, Service Level, and Health. World Health Organization; 2003. p. 1-39.
- Triono MO. Access Clean Water in the Community of Surabaya City and Their Bad Impacts Clean Water Access to Surabaya Community Productivity. Jurnal Ilmu Ekonomi Terapan 2018; 3(2):143-53. [ Google Scholar]
- Nurzanah TN, Wispriyono B, Anwar A. Sanitasi dan Air Minum di Daerah Perkotaan dan Pedesaan di Provinsi Bengkulu (Analisis Data Potensi Desa 2018). Jurnal Ekologi Kesehatan 2019; 18(3):159-70. [ Google Scholar]
- Labado N, Wulandari RA. Hubungan Sumber Air Minum dengan Kejadian Diare di Provinsi Gorontalo. Jurnal Medika Hutama 2022; 3(4):402-6. [ Google Scholar]
- Romlah SN, Puspita RR, Ratnasari D. Pendidikan Kesehatan dengan Media Video Memengaruhi Pengetahuan dan Sikap Anak dalam Pencegahan Penyakit Diare. Jurnal Kesehatan Pertiwi 2020; 2(1):118-24. [ Google Scholar]
- Katiandagho D, Darwel D. Hubungan Penyediaan Air Bersih dan Jamban Keluarga dengan Kejadian Diare pada Balita di Desa Mala Kecamatan Manganitu Tahun 2015. Jurnal Sehat Mandiri 2019; 14(2):64-78. [ Google Scholar]
- Aini N. Teori Model Keperawatan Beserta Aplikasinya dalam Keperawatan. Malang: Universitas Muhammadiyah Malang Press; 2018.